An editor has performed a search and found that sufficient sources exist to establish the subject's notability. (November 2022) |
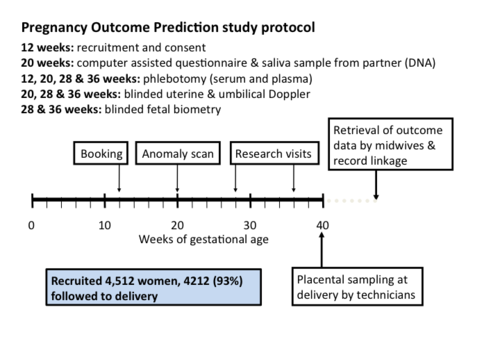
The Pregnancy Outcome Prediction (POP) Study[1] is a prospective cohort study of 4,512 women who have never given birth, recruited at the Rosie Hospital (Cambridge, UK) between January 2008 and July 2012.[2][3]
Staff and funding
editThe Principal Investigator is Gordon Smith[4] of the Department of Obstetrics and Gynaecology (University of Cambridge, UK). Lab work using the biobank of samples is led by Stephen Charnock-Jones[5] of the same department. The POP study is supported by the Women’s Health and Paediatrics[6] theme of the National Institute for Health Research (NIHR) Cambridge Biomedical Research Centre (BRC),[7] which is based at the Cambridge Biomedical Campus (UK). Other funding sources for the projects related to the POP study are the Medical Research Council (UK), the NIHR, the Wellcome Trust, the British Heart Foundation, and the Stillbirth and Neonatal Death Society (now known as Sands), as well as Industry supported studies.
Background
editIn 2007, Cambridge (UK) received funding from NIHR to establish a comprehensive Biomedical Research Centre (BRC). The Cambridge BRC Women’s Health and Paediatrics theme focuses on tackling the origins, treatment and prevention of many of the health issues that affect women during their reproductive years. The bulk of the Cambridge BRC funding for the first five years of the theme supported the POP study.
Over recent years, we have witnessed a great improvement in population-based screening methods for fetal abnormalities as a result of technological developments in ultrasound, biochemical screening and molecular genetics. However, the methods for screening the low risk population for other complications of pregnancy such as fetal growth restriction (FGR), pre-eclampsia and stillbirth have remained largely unchanged for the past 20-30 years. The UK National Institute for Clinical Excellence (NICE) has highlighted a number of research priorities in their guidelines for pregnancy care. These include a focus on improving the screening of apparently healthy pregnant women and identify those at high risk of complications. This area is the main focus of the POP study.
Design and aims
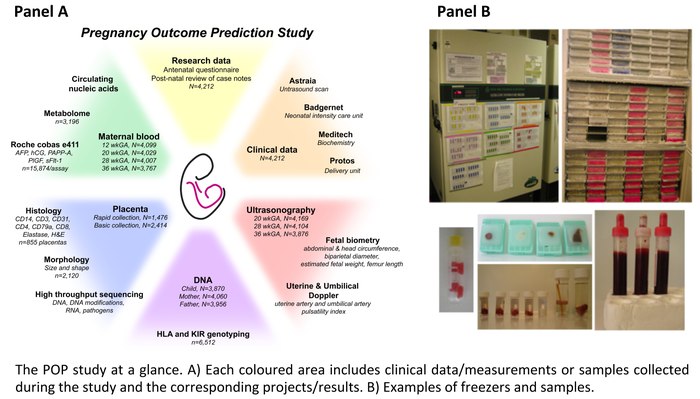
editNulliparous women with a viable singleton pregnancy were recruited to the POP study when attending their dating ultrasound scan at The Rosie Hospital (Cambridge, UK). The only clinical exclusion criterion was multiple pregnancy. Participants had serial ultrasound scans and blood obtained at recruitment, 20, 28 and 36 weeks of gestation. DNA samples and height/weight measurements of the partners were also collected. After delivery, biopsies of the placenta, placental membranes, umbilical cord, and a sample of cord blood were collected.[8] Thorough design of the POP study and careful sample collection allowed the creation of an extensive, optimally phenotyped biobank of complicated and healthy pregnancies, including approximately 230,000 blood and tissue samples stored in -80°C freezers, 24,000 formalin fixed placental biopsies, and 4,000 paternal DNA samples.
The types of samples collected during the POP study reflect, first of all, the focus on the role of the placenta and its altered development and function in several major complications of pregnancy. Second, they reflect the interest in circulating biomarkers since, despite years of intensive research, screening for these conditions is still largely based upon clinical grounds rather than ultrasonic and/or biochemical assessment of placental function. Therefore the projects based on the samples from the POP study have the following aims:
- understanding the mechanisms leading to placentally-related complications, such as pre-eclampsia, FGR and stillbirth;
- studying the association between pregnancy complications and the presence of infectious agents in the placenta;
- evaluating the performance of known biomarkers and serial ultrasonography in assessing maternal and fetal well-being;
- discovering novel, placentally-derived circulating biomarkers which reflect the underlying pathology and are highly sensitive and specific in predicting the associated disease.
Key findings
editMultiple projects based on this data have been published and many are currently on-going[as of?]. The key findings obtained so far studying the samples from the POP study are (see paragraph “Research papers” for a complete list of publications):
- Universal use of ultrasound to screen nulliparous women in the third trimester roughly triples the detection of small for gestational age (SGA) infants; moreover, combining ultrasound measurements of the estimated weight and of the growth velocity of a fetus identified a subset of small babies at increased risk of neonatal morbidity.[9]
- Maternal serum level of Delta-like homolog 1 (DLK1), protein involved in the regulation of maternal metabolic state and fetal growth in mice, differentiates constitutionally small and pathologically small (or fetal growth restricted) human fetuses.[10]
- Fetuses of mothers who developed gestational diabetes mellitus (GDM) grow faster already before the time GDM was diagnosed (women are typically screened at 28 weeks of gestation), suggesting that screening for GDM should be performed earlier (at 24 weeks).[11]
- A predictive model using blinded ultrasound estimated fetal weight (EFW) at 36 weeks, maternal age, height, BMI and weight gain correctly identifies women at increased risk of emergency C-section: in this study 48% of screen-positive women delivered by C-section.[12]
- Third-trimester screening of nulliparous women by universal ultrasound fetal biometry increases the detection rate of large for gestational age (LGA) infants and, combined with ultrasound measurements of fetal growth velocity, identifies those at increased risk of adverse neonatal outcome.[13]
- A clinically useful screening test for pre-eclampsia and FGR combines placentally-derived proteins measured in the maternal serum (i.e. the ratio of soluble fms-like tyrosine kinase 1 (sFLT1) to placental growth factor (PlGF)) and ultrasonic estimation of fetal weight.[14][15]
- The placenta exhibits a unique sex-dependent difference in polyamine metabolism, which is associated with placental-specific escape from X-chromosome inactivation by the enzyme spermine synthase (SMS); moreover, maternal serum levels of polyamine metabolites differ by fetal sex and strongly differentially associate with the great obstetrical syndromes, namely higher maternal serum levels of N1,N12-diacetylspermine (DiAcSpm) increases the risk of pre-eclampsia but decreases the risk of FGR.[16]
- A novel biomarker for pre-eclampsia, 4-hydroxyglutamate, improves current first-trimester prediction of the preterm disease.[17]
- Universal late-pregnancy ultrasound in nulliparous women could identify around 14,826 otherwise undiagnosed breech presentations across England annually and could, therefore, reduce emergency cesarean section and fetal mortality in breech presentation; moreover, it would be cost effective if fetal presentation could be assessed for less than £19.80 per woman.[18]
- The human placenta does not have a microbiome and placental bacterial infection is not a common cause of adverse pregnancy outcome; however, the placenta is a potential site of perinatal acquisition of S. agalactiae (group B Streptococcus), a major cause of neonatal sepsis.[19]
- A maternal serum metabolite ratio predicts FGR at term and approximately doubles the discrimination capacity between cases and controls as compared to the sFLT1:PlGF ratio.[20]
- The presence of inherited, chromosomally integrated human herpesvirus 6 (HHV-6) DNA in the feto-placental unit is associated with an 2-3 fold increased risk of the mother to develop pre-eclampsia; moreover, this study did not identify any other viral associations with pre-eclampsia and FGR.[21]
To externally validate the POP study findings, some of the above projects also involved collaboration with investigators from the Born in Bradford study.[17][20] Moreover, additional collaborations included the Cambridge University School of Biological Sciences (in particular, the Centre for Trophoblast Research,[22] a major international centre for placental research including >20 research groups), the Cancer Research UK (CRUK) Cambridge Institut and the Wellcome Sanger Institute. These studies also benefited from collaborations with industrial partners such as GE Healthcare and Roche.
Follow-up work
editPOPS2
editThe Pregnancy Outcome Prediction study 2 (POPS2) is a prospective cohort study funded by the Wellcome Trust. Recruitment to the study started in January 2020. The first POP study generated a simple screening test which is strongly predictive for pre-eclampsia and FGR at term. The test combines maternal risk factors, ultrasound measurements and levels of placentally-derived proteins in maternal serum (sFlt-1:PlGF ratio). The goal of POPS2 is to collect similar data and samples from approximately 4,500 unselected nulliparous women to address the following aims:
- to assess whether the test generated by the POP study works in an independent cohort;
- to nest a randomised controlled trial (RCT) of screening and intervention within the cohort in order to evaluate whether pregnancy outcome can be improved by inducing labour early (from 37 weeks) in women who screen positive;
- to collect more blood samples in order to develop and validate new predictive tests to detect a bigger proportion of pregnancy complications and to identify them earlier in pregnancy.
POPStar
editPregnancy Outcome Prediction Study: transgenerational and adults review (POPStar) is a follow-up study of the original POP study, conducted by the Department of Obstetrics and Gynaecology in collaboration with the Department of Paediatrics (both University of Cambridge). The study is funded by the National Institute for Health Research (NIHR) Cambridge Biomedical Research Centre (BRC) and the children’s charity, Action Medical Research.
POPStar looks at the long-term health and development of the children and the mothers of the POP study cohort. POPStar started in June 2020, when the children were between 8 and 12 year old. The study is based on the link between routinely-collected data (e.g. from the UK National Health Service and the Department for Education) and the results from POP study in order to determine which pregnancy parameters could predict a high risk of health or developmental problems. Using the existing and follow-up data collected during the POP and POPStar studies, the research team aims to make connections between conditions during pregnancy and current maternal and children health.
References
edit- ^ "The Pregnancy Outcome Prediction (POP) Study".
- ^ Pasupathy D, Dacey A, Cook E, Charnock-Jones DS, White IR, Smith GC (November 2008). "Study protocol. A prospective cohort study of unselected primiparous women: the pregnancy outcome prediction study". BMC Pregnancy and Childbirth. 8 (1): 51. doi:10.1186/1471-2393-8-51. PMC 2611961. PMID 19019223.
- ^ Gaccioli F, Lager S, Sovio U, Charnock-Jones DS, Smith GC (2017-11-01). "The pregnancy outcome prediction (POP) study: Investigating the relationship between serial prenatal ultrasonography, biomarkers, placental phenotype and adverse pregnancy outcomes". Placenta. 59: S17–S25. doi:10.1016/j.placenta.2016.10.011.
- ^ "Professor Gordon Smith".
- ^ "Professor Stephen Charnock-Jones".
- ^ "Women's Health and Paediatrics".
- ^ "National Institute for Health Research (NIHR) Cambridge Biomedical Research Centre (BRC)".
- ^ "Visual placental sampling demonstration". YouTube.
- ^ Sovio U, White IR, Dacey A, Pasupathy D, Smith GC (November 2015). "Screening for fetal growth restriction with universal third trimester ultrasonography in nulliparous women in the Pregnancy Outcome Prediction (POP) study: a prospective cohort study". Lancet. 386 (10008): 2089–2097. doi:10.1016/S0140-6736(15)00131-2. PMC 4655320. PMID 26360240.
- ^ Cleaton MA, Dent CL, Howard M, Corish JA, Gutteridge I, Sovio U, et al. (December 2016). "Fetus-derived DLK1 is required for maternal metabolic adaptations to pregnancy and is associated with fetal growth restriction". Nature Genetics. 48 (12): 1473–1480. doi:10.1038/ng.3699. PMC 5373434. PMID 27776119.
- ^ Sovio U, Murphy HR, Smith GC (June 2016). "Accelerated Fetal Growth Prior to Diagnosis of Gestational Diabetes Mellitus: A Prospective Cohort Study of Nulliparous Women". Diabetes Care. 39 (6): 982–7. doi:10.2337/dc16-0160. PMID 27208333.
- ^ Sovio U, Smith GC (July 2018). "Blinded ultrasound fetal biometry at 36 weeks and risk of emergency Cesarean delivery in a prospective cohort study of low-risk nulliparous women". Ultrasound in Obstetrics & Gynecology. 52 (1): 78–86. doi:10.1002/uog.17513. PMID 28452133.
- ^ Sovio U, Moraitis AA, Wong HS, Smith GC (June 2018). "Universal vs selective ultrasonography to screen for large-for-gestational-age infants and associated morbidity". Ultrasound in Obstetrics & Gynecology. 51 (6): 783–791. doi:10.1002/uog.17491. PMID 28425156.
- ^ Sovio U, Gaccioli F, Cook E, Hund M, Charnock-Jones DS, Smith GC (April 2017). "Prediction of Preeclampsia Using the Soluble fms-Like Tyrosine Kinase 1 to Placental Growth Factor Ratio: A Prospective Cohort Study of Unselected Nulliparous Women". Hypertension. 69 (4): 731–738. doi:10.1161/HYPERTENSIONAHA.116.08620. PMC 5344177. PMID 28167687.
- ^ Gaccioli F, Sovio U, Cook E, Hund M, Charnock-Jones DS, Smith GC (August 2018). "Screening for fetal growth restriction using ultrasound and the sFLT1/PlGF ratio in nulliparous women: a prospective cohort study". The Lancet. Child & Adolescent Health. 2 (8): 569–581. doi:10.1016/S2352-4642(18)30129-9. PMC 6473551. PMID 30119716.
- ^ Gong S, Sovio U, Aye IL, Gaccioli F, Dopierala J, Johnson MD, et al. (July 2018). "Placental polyamine metabolism differs by fetal sex, fetal growth restriction, and preeclampsia". JCI Insight. 3 (13). doi:10.1172/jci.insight.120723. PMC 6124516. PMID 29997303.
- ^ a b Sovio U, McBride N, Wood AM, Masconi KL, Cook E, Gaccioli F, et al. (February 2020). "4-Hydroxyglutamate is a novel predictor of pre-eclampsia". International Journal of Epidemiology. 49 (1): 301–311. doi:10.1093/ije/dyz098. PMC 7124498. PMID 31098639.
- ^ Wastlund D, Moraitis AA, Dacey A, Sovio U, Wilson EC, Smith GC (April 2019). "Screening for breech presentation using universal late-pregnancy ultrasonography: A prospective cohort study and cost effectiveness analysis". PLOS Medicine. 16 (4): e1002778. doi:10.1371/journal.pmed.1002778. PMC 6467368. PMID 30990808.
- ^ de Goffau MC, Lager S, Sovio U, Gaccioli F, Cook E, Peacock SJ, et al. (August 2019). "Human placenta has no microbiome but can contain potential pathogens". Nature. 572 (7769): 329–334. Bibcode:2019Natur.572..329D. doi:10.1038/s41586-019-1451-5. PMC 6697540. PMID 31367035.
- ^ a b Sovio U, Goulding N, McBride N, Cook E, Gaccioli F, Charnock-Jones DS, et al. (March 2020). "A maternal serum metabolite ratio predicts fetal growth restriction at term" (PDF). Nature Medicine. 26 (3): 348–353. doi:10.1038/s41591-020-0804-9. hdl:1983/7dd6b8f2-7ef5-4d7f-b71d-df9f9e32067e. PMID 32161413. S2CID 212668904.
- ^ Gaccioli F, Lager S, de Goffau MC, Sovio U, Dopierala J, Gong S, et al. (May 2020). "Fetal inheritance of chromosomally integrated human herpesvirus 6 predisposes the mother to pre-eclampsia". Nature Microbiology. 5 (7): 901–908. doi:10.1038/s41564-020-0711-3. PMC 7610361. PMID 32367053.
- ^ "Centre for Trophoblast Research".